Orthognathic Surgery: In a Multidisciplinary Way
Introduction:
Jaw Surgery (Orthognathic Surgery) is an operation to reposition the jaws. The operation corrects any imbalance between the skeletal component holding the teeth to create harmony and balance. The surgery will change facial looks. It also enables correction of the bite and dental aesthetics (such as a gummy smile, lack of incisal show etc).

“I have never been happy with my smile, I would like a new smile, a good bite and a balanced profile”
Case:
25-year old female referred to improve facial appearance and occlusion.
Findings:
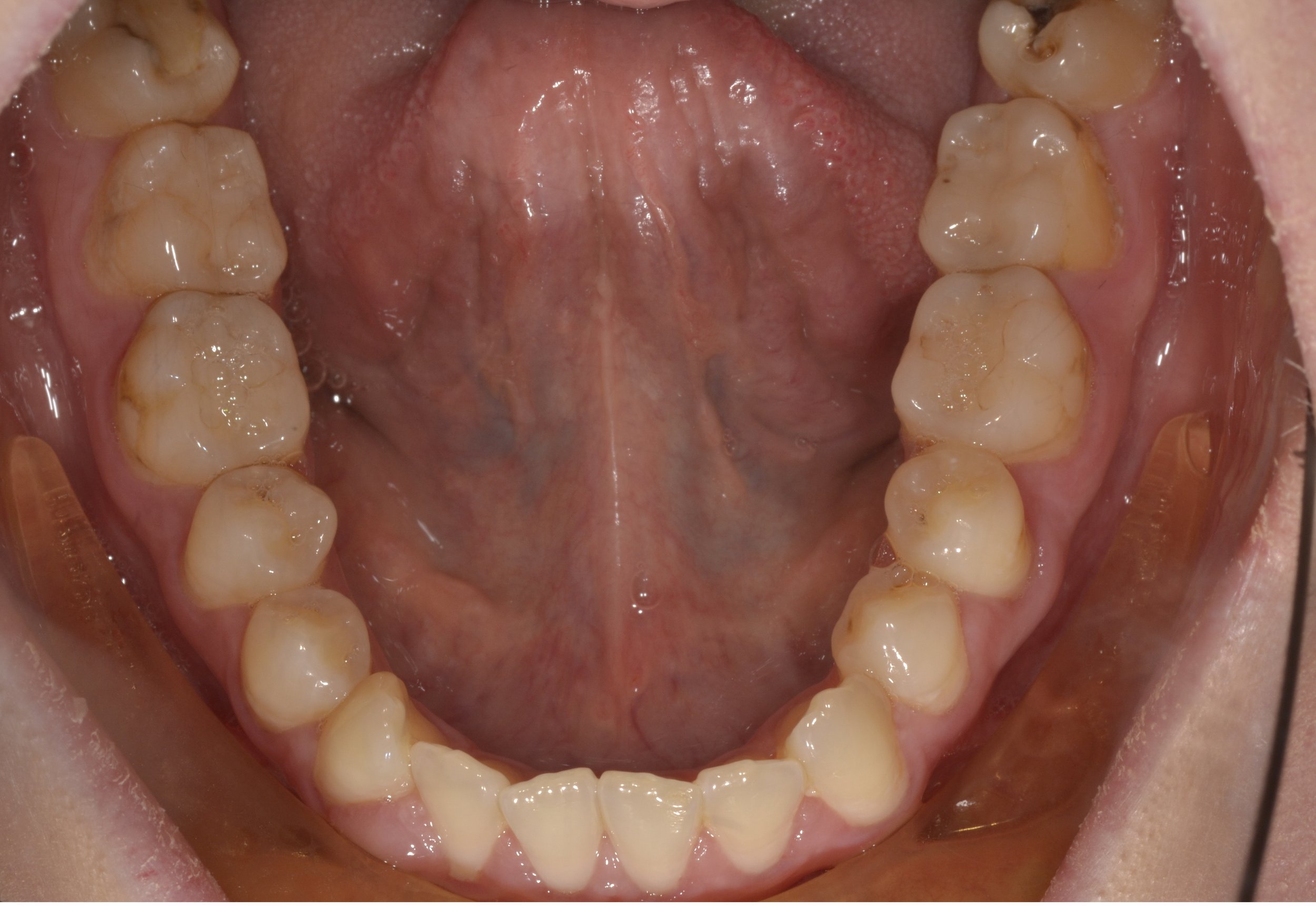
• Maxilla hypoplastic in an antero-posterior/transverse plane.
• Mandible prognathic and asymmetric to the right.
• No incisal show at rest.
• Anterior open bite: contact on molars only.
• Upper arch canted (lower on the right).
• Severe upper crowding and undersized upper incisors (Bolton’s discrepancy).
• Crossbite due to skeletal positions.
• TMJ – click on the right side. No deviation/good mouth opening.
• All wisdom teeth present and erupt.
• Some old, discoloured composite restorations especially on the upper anterior teeth.
Goals
1. Facial balance.
2. Stable occlusion with normalised overate/overbite.
3. Dental/smile harmony.
4. Dental/gum health.
5. Stable Temporomandibular Joint (TMJ).
Treatment Options
1. Orthodontics with the extraction of upper first premolars and lower third molars. Bimaxillary orthognathic surgery with segmented three piece
maxilla. 36-month treatment length.
2. Upper orthodontics only (non-extraction). Bite not corrected/No facial changes. 15-month treatment length.
3. No treatment.
Mechanics and Treatment
Option 1
1. Extraction of upper first premolars and lower third molars. Upper and lower fixed labial appliances.
2. Alignment/normalise torque of lateral segments.
3. Space distal to upper laterals for segmental cuts.
4. Bonding of the upper third molars for bite control.
5. Digital surgical planning.
6. Bimaxillary surgery - Upper jaw 3-piece segmental surgery for advancement and traverse control. Lower jaw.
7. Post- surgical bite settling/detailing.
8. Post orthodontic restorative work - Change composites.
- Veneer’s upper 2 to 2.
- Composites upper 3’s.
9. Retention: Lower fixed retainer and upper and lower night-time vacuum formed retainers.
Key Points
• Correct diagnosis.
• Collaborative orthodontics/surgery/restorative communication throughout treatment.
• Three-piece maxilla for transverse correction. Surgically assisted rapid palatal expansion (SARPE) was not required.
• Stabilisation of the bite immediately post-surgery with molar compomers is essential. This maintains the bony segments and prevents the distortion/flexing of the skeletal segments.
• Upper third molars were kept as the upper first premolars had been extracted and the maxilla was moved forwards in the surgical phase. Therefore, the upper third molars were brought into occlusion.
• Stability is key: long term retention is imperative.








PRE TREATMEnT









Mid treatment









FINAL RESULTS
“They feel just like my own teeth, just a part of my smile now. I love them!”